Q&A Report: Opening a New Window: Stable Long-Term Imaging of Dura Mater–Transplanted Pancreatic Islets in Awake Mice
The answers to these questions have been provided by:
Philip Tröster, PhD
Scientist
Rolf Luft Research Center for Diabetes and Endocrinology
Department of Molecular Medicine and Surgery, Karolinska Institutet
Martin Köhler, PhD
Scientist
Rolf Luft Research Center for Diabetes and Endocrinology
Department of Molecular Medicine and Surgery, Karolinska Institutet
Do the mice need to be kept in single housing or is it possible to keep them in group housing with the head-set?
Neurotar: In addition to supplying head-fixation solutions to academic labs, Neurotar performs in vivo two-photon and wide-field imaging studies for pharmaceutical and biotech partners and operates under an animal license issued by the Finnish Animal Board. Based on this experience, mice with implanted head plates can be group-housed in standard laboratory cages. In our experience:
- Head plates do not detach
- Head plates do not get stuck in cage bars
- Mice do not remove their own or their cage mates’ head plates
Group housing reduces stress and supports normal behavior. However, we do not recommend mixing mice with and without head plates in the same cage. Group housing is allowed under the Neurotar license.
PT/MK: Group housing has shown no difficulties or problems and is encouraged by our permit, as it improves animal welfare and reduces stress. Mice are only housed individually for up to one week after surgery to allow for recovery. After this period, group housing is resumed. Whenever possible, we use female mice that were housed together prior to cranial surgery or males from the same litter to ensure compatibility. Depending on availability, animals are housed in pairs or groups of three.
With the window on the head, the brain receives more light - did this change brain/neurons activity below the window or does the islet cover the brain sufficiently to avoid increased light-exposure?
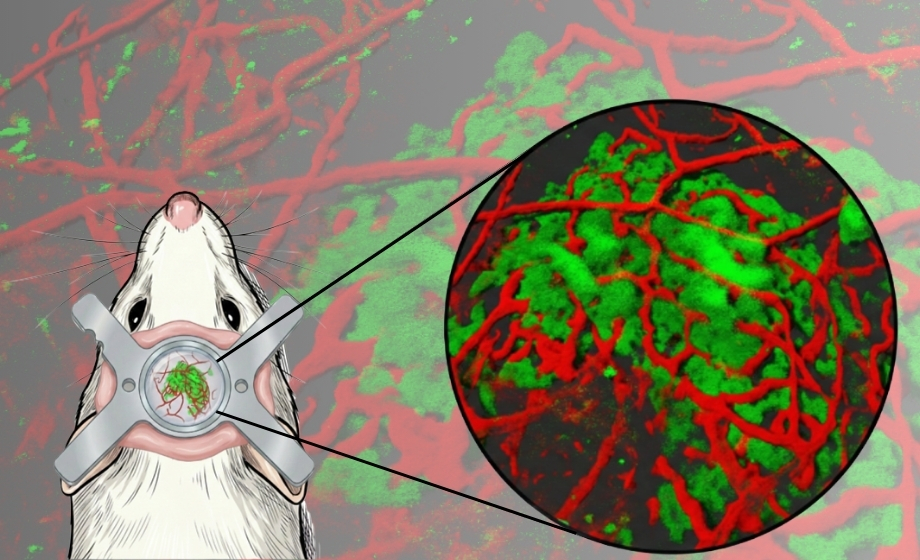
PT/MK: Dura mater-engrafted pancreatic islets do not provide sufficient coverage of the brain surface: standard transplantation (~10 islets) covers only ~10–20%, and even higher-density transplantation (~50 islets) does not fully cover the cranial window. Thus, they cannot act as a meaningful light barrier.
- Although the glass coverslip and the semi-translucent dura mater allow some light penetration to the superficial cortical layers, typical ambient room lighting (100–300 lux, diffuse) has been tolerated in our experiments and is considered non-influential. Confocal imaging was conducted in a dark environment, with only indirect, dim light sources positioned away from the cranial window.
- Potential light effects remain a valid consideration, particularly for studies investigating neuronal innervation of transplanted islets. To minimize any unwanted prolonged light exposure, the cranial window can be covered with opaque material (e.g., duct tape) supported by the head plate. This approach is also planned for experiments using optogenetic tools to ensure a fully protected baseline prior to controlled stimulation.
How can you make a cranial window last for a long time? Wouldn't It just blur after a month or so? Are there any tips you can provide?
Neurotar: Cranial windows often become partially opaque during the first weeks after surgery due to inflammation, but transparency frequently improves after 3-4 weeks. Long-term success depends on surgical technique and experience. At Neurotar, 50–80% of windows remain suitable for long-term imaging. Mice with chronic windows are typically maintained up to one year in our facility.
Neurotar users receive free access to 13 cranial surgery protocols (videos) and handling and training recommendations via the customer portal.
PT/MK: The main factor is certainly the refinement of the surgical procedure. This allowed us to monitor engraftment and revascularization weekly during the first month, with awake imaging typically performed between 1 and 4 months after surgery. We never had issues with transparency, but we occasionally observed bone regrowth, which in some cases reduced the cranial window area by up to ~30%.
Key surgical considerations:
- Strict sterility and minimization of tissue trauma are essential to prevent micro-infections and inflammation. During skull drilling, heat and friction can induce inflammatory responses and bone necrosis. To mitigate this, we drill slowly in short bursts with intermittent pauses, while continuously cooling the area using a pointed air stream delivered through a flexible tube fitted with a 1-mL pipette tip, which also helps maintain a clean surgical field. The total drilling time, including pauses, is approximately 20 minutes.
- Thorough irrigation prior to coverslip placement is essential. Before introducing the islets and sealing the cranial window, the chamber is repeatedly rinsed with chilled Ringer’s solution to minimize micro-bleeding. Residual blood can otherwise promote immune activation, including macrophage recruitment, which may compromise both tissue health and long-term optical clarity.
Did the animal care committee have concerns surrounding the experiment/procedure?
Neurotar: Neurotar operates under a license issued by the Finnish Animal Board, reviewed and renewed annually since 2011. Chronic imaging is commonly approved when proper analgesia, recovery, and habituation are used. Longitudinal imaging reduces the number of animals used in experiments, which is viewed favorably by animal care committees.
PT/MK: Yes. Prior to obtaining full ethical approval, we first conducted a pilot study. The primary concerns raised by the animal care committee related to long-term brain health following transplantation and the use of awake imaging, which involves restraint and is classified as a critical procedure.
- A strict animal welfare scoring system was implemented, with a slightly elevated intervention threshold of 0.6 points during the first five postoperative days, during which analgesia could be administered. Thereafter, humane endpoints were set at 0.4 points, marginally above the baseline level of 0.3 applicable to non-experimental animals.
- In addition, we demonstrated that the five-day habituation protocol prior to awake imaging significantly reduced stress, as reflected by decreased stress-associated blood glucose levels.
- Overall, the study was positively evaluated in relation to the principles of the 3Rs.
How did you get two color imaging?
PT/MK: Two-color imaging was achieved by combining distinct excitation wavelengths with separate detection channels, together with specific fluorophores and genetically encoded sensors.
- For structural z-stack analysis, images were acquired sequentially by alternating between the green and red channels on a confocal microscope. Excitation was performed at 488 nm and 561 nm, with emission collected using dedicated HyD detectors and appropriate spectral separation to minimize bleed-through. The 488 nm laser was used to excite the GCaMP3 calcium indicator, while the 561 nm laser was used for visualization of lectin–dextran following intravenous injection for vascular labeling.
- For fast imaging of red blood cell dynamics, a resonance scanning mode (55.5 fps) was employed. In these experiments, green and red channels were acquired simultaneously in non-sequential mode to capture rapid physiological changes. The 633 nm far-red laser was used to excite DiD-labeled red blood cells, while the 488 nm laser enabled visualization of FITC–dextran for vascular contrast.
Don't the mice grow over time?
Neurotar: Chronic cranial windows are typically performed in adult mice (from ~2 months of age), when skull growth is minimal, and size is stable – an important parameter for surgery. In operated mice, partial skull regrowth may occur at the window edges over time, gradually reducing the usable imaging area. However, longitudinal imaging usually remains feasible in selected regions.
In developing mice, chronic windows are generally not recommended before the skull is sufficiently solid and the size is stable. Acute windows have been reported from around P8, and longitudinal windows from ~P16 in collaborating labs.
PT/MK: The youngest animals we initially tested were 2 months old; however, we subsequently increased the minimum starting age to avoid complications related to ongoing skull growth and potential loosening of the head plate. Currently, we primarily use mice at approximately 12 weeks of age, with body weight adjusted for sex and strain, corresponding to full adult skeletal maturity.
Have you tested oral food intake to assess calcium activity in islets on the dura mater?
PT/MK: Yes, this is an important and very interesting direction. We are currently testing oral glucose delivery paradigms, including sugar pellets as well as a modular lick-port system adapted for the Mobile HomeCage, which allows administration of glucose/sucrose solutions during awake calcium imaging of the dura mater–engrafted islets. This approach provides an opportunity to probe islet activity in a more physiologically relevant context, spanning from nutrient intake to β-cell activation.
However, a current limitation is the lack of continuous blood glucose measurements in the same experimental setting, which prevents precise temporal alignment between systemic glycemia and the onset of islet graft activity. We are therefore actively exploring complementary monitoring strategies to address this, as well as systematically comparing water versus sugar-water conditions to better define stimulus–response relationships.
After the 5-day habituation, did you observe any chronic stress effects on systemic glucose metabolism long-term?
PT/MK: No, we did not observe any signs of long-term metabolic or behavioral abnormalities following the five-day acclimatization period. Aside from expected age-related changes, the pancreatic islets engrafted onto the dura mater exhibited stable calcium activity beginning approximately 2–3 weeks post-transplantation, corresponding to the period of vascular integration, and maintained normal tissue behavior for several months up to the end of the experimental period.
- To further minimize potential cumulative stress effects, imaging sessions were spaced at intervals of at least one day. In cases where awake imaging was interrupted for longer periods, repeating the cage acclimatization phase appeared beneficial to re-establish stable behavioral adaptation.
During intravital imaging in awake mice, did you consider using telemetry implants or a mouse-adapted CGM to continuously monitor blood glucose in real time?
PT/MK: Yes, we have considered this, as continuous blood glucose monitoring would be highly valuable for interpreting islet calcium dynamics in relation to metabolic demand.
- Telemetry-based implants requiring vascular access (e.g., aortic placement) are not feasible in our setting due to surgical complexity and ethical constraints on invasive procedures.
- Subcutaneous continuous glucose monitoring (CGM) is a more practical approach and is something we plan to explore.
- In addition, we are considering genetically or chemically encoded glucose-sensitive fluorescent sensors in the graft or surrounding tissue, which could provide a minimally invasive, dynamic readout of systemic glucose fluctuations and enable correlation with β-cell calcium activity.
What is the maximum longevity of the cranial windows before optical clarity degrades or fibrous encapsulation occurs?
PT/MK: In our practice, most imaging experiments were completed within 4–6 months after transplantation without any significant loss of optical clarity or evidence of fibrotic capsule formation. In several cases, we were able to image animals up to 9–10 months post-transplantation; during this period, the islet cells remained optically accessible at the dural surface and exhibited preserved calcium signaling activity, alongside stable optical clarity of the cranial window.
- In some instances, we observed a gradual reduction in the effective imaging area, most likely due to peripheral bone regrowth encroaching from the edges, rather than any deterioration of the central optical window.
Are the parasympathetic and sympathetic networks in the graft functionally active? Can they dynamically modulate insulin secretion?
PT/MK: At present, we do not yet have functional evidence for autonomic modulation of the graft. We have only demonstrated morphological integration of nerve fibers within the islet grafts, without direct assessment of sympathetic or parasympathetic functional activity or its impact on insulin secretion. This remains an important question that we aim to address in future experiments.
However, it is well established that in native pancreatic islets, parasympathetic innervation, particularly via acetylcholine acting on muscarinic receptors on β-cells, can significantly modulate insulin secretion. Whether this physiological neuroendocrine regulation is functionally re-established in our graft system remains to be determined.
Do you plan to use the xenotransplantation model to test novel diabetes drug efficacy and local toxicity longitudinally?
PT/MK: Yes. We aim to further develop the cranial window platform as a longitudinal in vivo drug-testing system, enabling functional readouts of graft physiology over time. A key advantage of this approach is the ability to directly monitor tissue-level responses to therapeutic interventions in a stable, repeatable imaging setting. In particular, we plan to combine pharmacological testing with diet-induced metabolic challenges to assess efficacy under physiologically relevant conditions.
Could this system monitor real-time beta-cell Ca²⁺ signaling degradation during diet-induced T2D progression?
PT/MK: We believe this is feasible. Functional readout studies in alternative ectopic transplantation sites, such as the anterior chamber of the eye, have demonstrated that high-fat and high-sucrose diets induce adaptive changes in islet morphology and calcium signaling. We anticipate that similar dynamics should be detectable in the dural islet transplantation model. In fact, this platform may offer additional advantages due to improved mechanical stability, higher-resolution longitudinal imaging, and the ability to study awake physiology, which together enable a more comprehensive assessment of β-cell calcium dynamics during diet-induced progression toward type 2 diabetes.
What originally led you to try the brain as a transplantation site for pancreatic islets?
PT/MK: Our primary motivation was to enable the study of pancreatic islet physiology under fully awake, unanesthetized conditions. Anesthesia is well known to significantly alter cellular responses to metabolic stimuli, which can confound measurements of islet calcium dynamics and insulin secretion. Therefore, we sought an approach that would allow us to investigate these processes under minimally perturbed physiological conditions.
By combining dural islet transplantation with the Mobile HomeCage system, we were able to achieve both optical accessibility and the absence of anesthesia-related artifacts. Importantly, the exceptional mechanical stability of this setup, critical for single-cell–resolution imaging, emerged as an additional advantage.
What were the key factors that allowed you to achieve stable long-term imaging in awake mice?
PT/MK: Stable imaging during awake sessions was achieved through a combination of factors:
- Proper animal habituation was essential to minimize resistance and promote calm, stress-free behavior with smooth, natural movements during imaging.
- Maintaining a clean setup, particularly avoiding residual liquid or debris from immersion media, was critical for imaging stability.
- Equally important was a robust and well-optimized head-plate implantation, using sufficient dental cement to ensure rigidity. We also found that smaller head-plate designs provided better stability; in our hands, sizes #3 was optimal.
- Combining rigid head fixation with the Mobile HomeCage system minimized motion artifacts while preserving natural behavior, enabling stable single-cell–resolution imaging over sessions of up to 90 minutes.
Do you see this transplantation approach being used for other tissues or organoids?
PT/MK: Yes, absolutely. Ectopic transplantation of tissues and organoids is well-established across multiple sites. Pancreatic islets are the perfect proof-of-concept: they are known to engraft successfully in the subcutaneous space, under the kidney capsule, and in the anterior chamber of the eye. The key argument is that if a tissue or organoid survives at these established ectopic sites for islet transplantation, it should equally survive on the dura mater. Building on this, we plan to test stem cell-derived islet organoids and other diabetes-related tissues as candidates for dura mater engraftment.
What advice would you give to researchers considering moving from anesthetized to awake imaging?
PT/MK: The cranial window surgery is technically demanding and requires practice, as does animal handling, which differs substantially from anesthetized or ex vivo imaging. However, the learning curve is manageable. We recommend a stepwise approach: first perform imaging under anesthesia at the new site to familiarize yourself with the microscopy settings and tissue characteristics, then habituate animals to the Mobile HomeCage independently before combining both elements in awake confocal imaging sessions. Prior experience with cranial window preparations is helpful but not a prerequisite.
Regarding animal ethics: keep experimental procedures as simple and clearly defined as possible when drafting the ethical permit application, as complexity in the protocol can complicate approval.